
This protocol can reverse brain atrophy
How immunity, lipids & membrane physiology collaps and what to do about it

One day when browsing on twitter I came across this picture (many thanks to Dr.T on X for nudging me on this deep rabbit hole):

On this we can see reversal of brain atrophy by a certain supplemental compound. I was intrigued as apart from bloating & constipation, brain fog is the third main symptom I suffered from.
Deeply I know that my underlying issues drive some form of brain atrophy. If you are me, you really do not want any neuro-inflammation happening, as its the opening event happening in all neurodegenerative diseases:
Dementia
Autonomic Issues
Parkinsons Disease
Alzheimers Disease
Any Cognitive Impairment
For many this begins with a long list of mild symptoms often deemed “unworthy” of treating:
Brain Fog
Dysautonomia
Memory issues
Loss of fluency
Puffy, heavy face
Hypersensitivity
ADHD like symptoms
Depression like symptoms
Headaches & migranes (not always though)
You’re not depressed, you’re inflamed
I dove into the science behind the protocol and what that led me to was nothing short of amazing. I potentially look at a protocol which could be a no brainer for many, many patients to restore proper function of the whole organism.
So, I wanna share what I found with you.
In this one, we will dive into how immunity, peroxisomes and membrane signaling are common pathways disrupted through toxin overload and what to do about it.
Let’s dive in.
Peroxisomes & Plasmalogen Science
When diving into the research, the first compound I came across (which was used in the studies above) where plasmalogens (PLs).
Our membranes are a bi-layer of phospholipids. These lipids have the special ability to be lipophilic (fat loving) while also being hydrophilic (water loving). Bi-layers of these lipids allows membranes to develop.

20% of these phospholipids are called plasmalogens. Especially enriched are the heart, brain & immune cells .What makes plasmalogens different to other phospholipids is their chemical structure:

They got an ether bond at the sn-1 position (called vinyl-ether bond), increasing electron density locally, giving them special properties.
These phospholipids are very important, which we can see from the most extreme cases of plasmalogens deficiency: Zellweger syndrome
Kids born with this genetic disease have disrupted peroxisomal metabolism, one of the main hubs for plasmalogen synthesis. The issue is a loss of these phospholipids while accumulating very long chain fatty acids (VLCFAs) which are neurodegenerative themselves.
True ZD kids will die within the first year, “milder” Zellweger spectrum disorders allows life up until early 20s (maximum). This gives clues into how important plasmalogens are, but what is there function?
Here is where it gets really interesting:
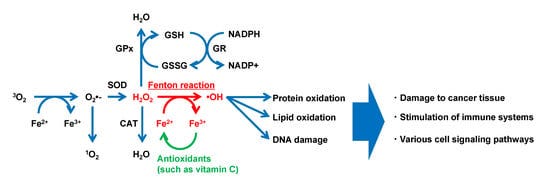
The biochemical properties allow for certain qualities not present in other phospholipids. First, they have excellent antioxidant capacity, protecting the membranes from lipid peroxidation by ROS, disrupting the vicious cycle of ever increasing radical formation.
Plasmalogens have the ability to influence membrane trafficking at neurons. Science shows that depletion of plasmalogen disrupts proper neurotransmission at synapses.
They accumulate at the synapatic shaft to allow vesicles to traffic metabolites & neurotransmitters into & out of the synaptic sheft. After all, within the brain PLs accumulate heavily, making up to 90% of myelin phospholipids.

Though being very important in this regard, their most interesting function for me is within the immune system:
Plasmalogens store long chain fatty acids, most notably DHA (n-3) and Arachidonic Acid/AA (n-6). These two unsaturated fatty acids are of utmost importance when it comes to shaping the inflammatory environment surrounding cells.
Whenever pathogens enter the cells, innate immunity increases ROS signaling & membrane turnover.
PLA2, an enzyme, releases these fatty acids which by themselves influence the inflammatory environment:
AA = pro & slightly anti-inflammatory
DHA = resolving inflammation
We need both to house a proper inflammatory response with resolution. Hence why the ratio of omega 6:3 should be < 4:1. Higher ratios than that tilt the immune system towards inflammation, without proper resolution.
Increasing evidence points towards even more functions within plasmalogens:
Loss of plasmalogens drives immunosuppression
Case reports of people with Zellweger syndrome show profound thymic atrophy, neutropenia & overall loss of white blood cells.
They increase phagocytosis of macrophages while also being of utmost importance in cellular metabolism of other white blood cells. Expression of MHC molecules is also dependent on re-shaping membranes, so plasmalogens play a role here, potentially inducing autoimmunity.
Maturation of CD8+ (cytotoxic T-cells), which are often downregulated under chronic antigenic load needs plasmalogens.
Low childhood levels of plasmalogens are associated with onset of T1D.

Even further, in the case of gut health, PLs lower TLR4 expression essentially lowering the effect of ongoing LPS challenge. This lowers inflammation and can lead to profound healing of the gut ecosystem.
Bile formation is dependent on PL synthesis which shapes the metabolic & gut landscape, tying further into the gut connection.
You now can grasp the amount of processes PLs support as they are inherently important for the membrane & cellular organism. But, is it really that affected under unhealthy conditions? if so, whats the mechanism here?
Here is where I made a huge connection:
Infections &Peroxisomal Dysfunction
After the age of 40, we loose up to 40% of Pls.
Loss of PLs and the amount of that loss is associated with worsening of Alzheimers and can even predict impairment & progression of the disease.
There is a whole list of neurodegenerative and behavioral disorders where a therapy of Pls might be helpful:
Multiple Sclerosis
Parkinsons Disease
ADHD or other related diseases
Even depression or other mood disorders
In menopausal women we can see white matter atrophy & ongoing myelin catabolism, as estrogen seems to be important in these processes. As 90% of phospholipids within the white matter could be PLs, a loss of it seems logical.
Metabolic diseases like T2D or CVDs are associated with disrupted lipid & membrane metabolism. PLs can restore lipid levels as they are important in the function of the lipoproteins (HDL, LDL) and their respective cellular uptake mechanisms.
Within the heart, special PLs formed with choline are found and loss of these is associated with myocardial infarction & stenosis.
But the most interesting one I found was this study:
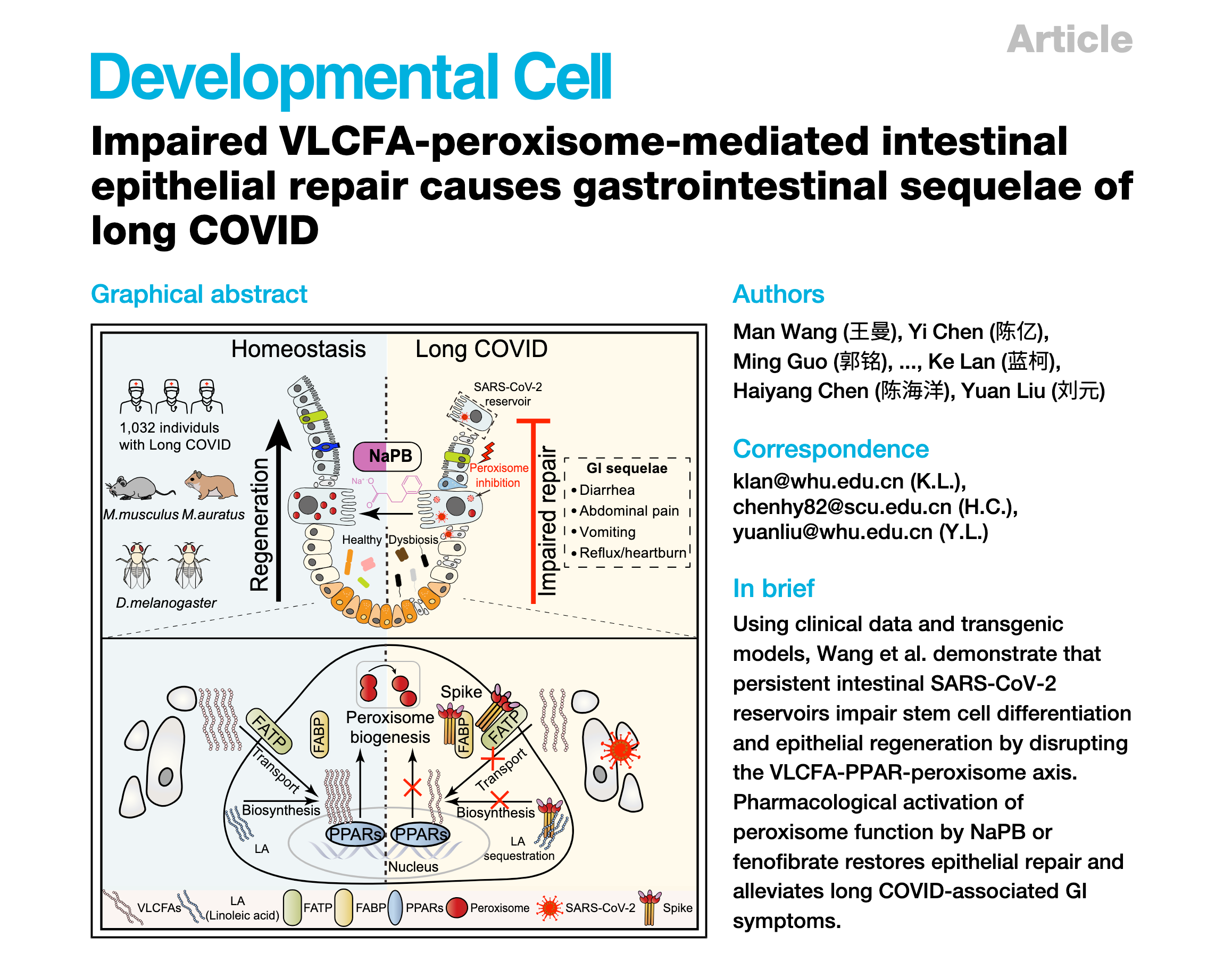
Long Covid is associated with massive loss of Pls, not only within the brain which could tie into the ongoing neuro-inflammation (& its symptoms), but also within the epithelial lining of the gut.
How can this happen?
Through disruption of the mitochondrial-peroxisomal axis
Peroxisomes where once thought to be little organelles not really that important in whole cell metabolism.
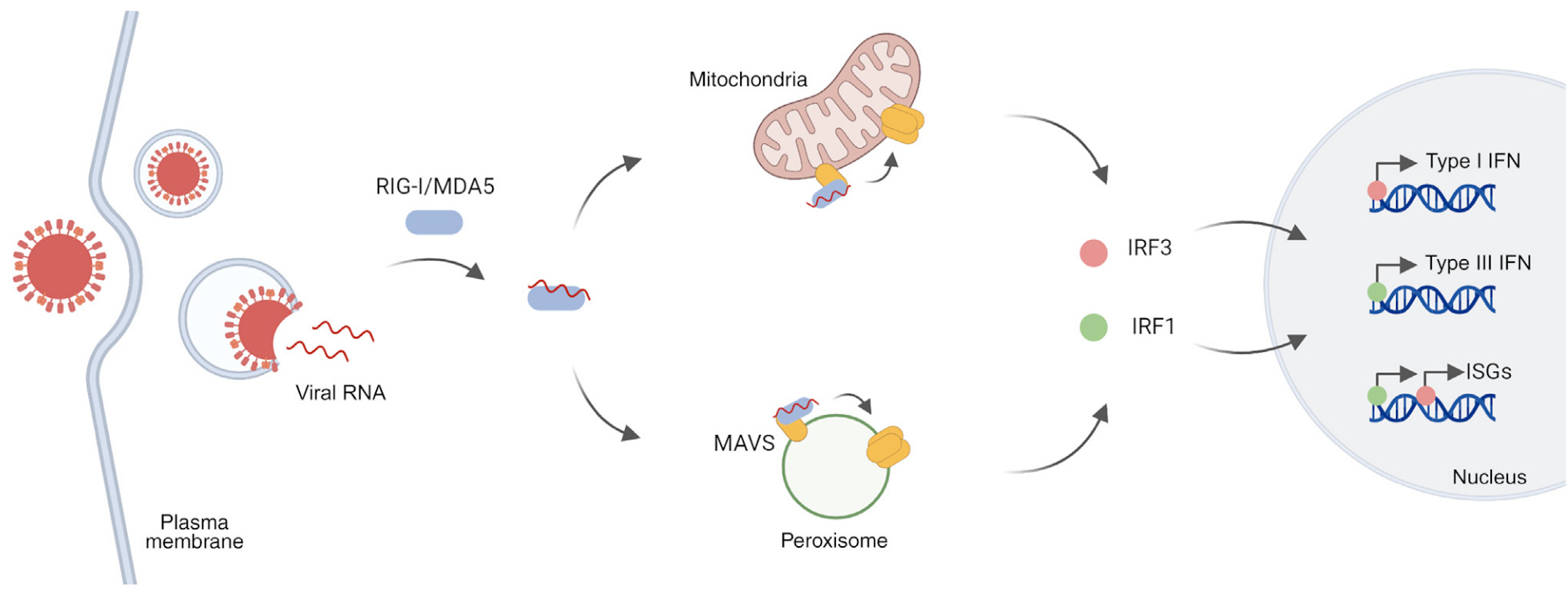
But then I came across a paper showing something remarkable:
Mitochondria directly connect to peroxisomes, offloading ROS into the cytosol of the peroxisome for further metabolism. As these organelles are high in mono- & dioxygenases, peroxisomes steer the ship of cellular redox.
Any entry of viral cells will lead to an increase in ROS, which is needed to destroy the entry of the virus. This is Th1 immunity in a nutshell.
Mitochondria & peroxisomes both play a huge role, not only through regulating said ROS levels, but also through genetic transcription mechanisms. When a virus enters a cell there is an orchestrated interplay between MTs and peroxisomes, which at the end induce a shift in immunity to fight off that pathogen.
But what seems to happen in Long Covid, as with other viruses, is that the immune activity is not enough to get hold of the virus. Persistent viral load within the gut lumen has already been found in humans with LC symptoms.
Viruses know that peroxisomes are of utmost importance in viral defense, hence why they hijack the peroxisomes:
Viruses can use the machinery of plasmalogens for their own replication
Viruses can stop the normal metabolism all together
Viruses can stop plasmalogen synthesis
Studies show peroxisomal disorders of LC patients within immune cells, the gut & the lungs. Other studies show potential links to Alzheimers. Peroxisomes are under attack in many, if not all, diseases through the relationship to the mitochondria & overall cellular redox milieu.
But what does that specifically mean for PL synthesis?
The rate limiting step of PL synthesis is the addition of a long chain fatty alcohol, which is happening right within the peroxisomes.
Entry of viruses into the cells where this happens means that there is loss of peroxisome function and PL synthesis.
The loss of peroxisome function has another big problem:
Accumulation of VLCFAs
These are normally burned by peroxisomes, but in these instances they cannot. Accumulation of these fatty acids is associated with neuroinflammation. It seems that these VLCFAs destabilize the membranes.
Loss of PLs + accumulation of VLCFAs = loss of membrane fluidity & integrity.
To summarize this part:
Viruses are known to hijack peroxisomes, leading to dysregulation of redox & lipid metabolism.
Not only increases in inflammation, but also loss of PL formation & membrane make up can be found, leading to dysfunctional cellular metabolism associated with all the functions of PLs above.
On top of that inflammation drives PL loss by itself:
Inflammation robs your Plasmalogens
A short side quest I wanna embark on is the role PLs play in buffering ROS, but also how exactly inflammation lowers these:
Think of Pls as ROS bufferers, as they are extremely good at oxidizing. Sounds counterproductive, right? But thats good, as they protect the membrane lipids from peroxidation, while their radical end products do not part take within further oxidation reactions.

Above you can see a “normal” cycle of peroxidation, where the peroxyl radical in itself supports the formation of further radicals. This cycle ends if plasmalogens are the sites of attack.
The next reason is also seen in exitotoxicity, immune activation or overall inflammatory milieus:
Entry of Ca2+ within a cell will lead to up regulation of PLA2, an enzyme which can catalyze reactions of the phospholipid bi-layer.
Normally known to release AA into the cytosol to support inflammatory processes its also a well known cleaver of Pls, leading to the formation of Lysoplasamlogens. These can be used to produce Pls after inflammation resolution or are by themselves promoting pro-inflammatory immunity in the acute phases.
")
Within neurons this process is massively altered by a shift in the GABA:Glutamate ratio (towards the latter), while also having overactive glutamatergic receptors.
Glutamate when binding to its receptors acts excitatory, especially when binding to NMDA receptors. This leads to an increase in Ca into the cell, leading to said mechanisms.
Excess glutamate is linked to mitochondrial damage, neuronal apoptosis, inflammation & downstream of that many neurodegenerative diseases.
Speaking of apoptosis, the last way we can loose PLs is through excessive apoptosis. Under apoptotic conditions mitochondria release cytochrome c as an intracellular trigger for apoptosis. Its well known that cytochrome c itself can act on membranes as a phospholipase, cleaving of PLs and their respective fatty acid at the sn-2 position.

This loss of PLs is also one reason, with general peroxidation of PUFAs, leading to the stiffening up of membranes found under toxic conditions (mold overload, viral load, bacterial infections,…). Its a well known phenomenon in functional medicine, which is a protective mechanism of the cell while downstream effects on proper cellular metabolism happen.
Membrane stiffness is determined by the ratio of saturated fats to unsaturated fats within the phospholipids. This is further optimized by cholesterol.
Up until now we covered three important questions:
What are plasmalogens?
Why are they important to us?
What happens under inflammatory conditions?
How does the peroxisomal-mitochondrial axis work under these conditions?
The more interesting question for you:
How can we change that?
Whats the protocol?
Let’s find out.
Apothecary: Implementing a LPR Protocol
To really understand said protocol, I often add theoretical blocks under certain compounds for you to grasp the theory. The protocol is divided into two parts:
Phase: 2-6 weeks of foundational work
Phase: ongoing LPR protocol for your case
But, for whom is such a protocol needed?
After research it, I came to the conclusion that there are a lot of people benefitting from it, but it would not be my main priority for all of them. The first I can think of are these conditions:
Long Covid & other viral exposures
Any neurodegenerative disorder (AD, PD, MS)
Mycotoxin injury (due to their accumulation in membranes)
Any other neuro-psychological disorder (depression, ADHD, bipolar disorders)
These are the 4 main ones where you definitely should think about it, but with that said, really any chronic inflammatory disease can use a phase of this.
Let’s start with the foundations.
Phase 1: Calming the cytokine storm
The first phase is for those who do not had any prior protocol done for their issue, for all others read it and see what you have been doing and what not. Its really important
Goals of this phase:
lowering inflammation so that the PLs can be incorporated properly
co-factor saturation to protect the membranes
overall stabilization of your physiology will reap benefits for any protocol
As I dabbled with a lot of other stuff on this newsletter already, or on my X account, I will keep this to the minimum to not be repetitive.
Due to their inherent nature, PUFAs like omega-3s are easily oxidized by ROS if we ingest them without their natural structure (like in fish). Also, the peroxidation risk under inflammatory conditions is higher compared to saturated fats.
There are certain micronutrients that we need to protect our membranes. Often these are associated with being or supporting anti-oxidant processes within the body.
Focus on these through diet or supplement:
Vitamin C (any fruit like berries, citrus or herbal teas like hibiscus)
Vitamin E (red palm oil or supplement)
Taurine (fish + supplement)
Iodine (daily fish OR seaweed will do the trick)
Selenium (brazil nuts, (organ) meats)
Zinc (red meat, oysters, any other (organ) meats; huge fan of supplementation)
A standard anti-inflammatory diet which I always recommend should be done. Its nothing special in this regard as we want maximum nutrient saturation while lowering inflammatory responses to food.
Meats, fish, eggs, organs, olive oil, coconut oil, butter, carrot, olives, zuchhini, berries and certain fruits are my go to recommendation. If tolerated rice or sweet potatoes. Bone broth, kefir & fermented foods if you do not have mast cell issues.
This will get you very far if you care to eat organs consistently. Else, a B-complex to fill up B2/3/6/7/9 and also some molybdenum would not hurt.
Supplements to further downregulate inflammation:
NAC/NACET + Glycine for glutathione
Boswellia + Curcumin + PEA is a great combination (2 of them are enough)
Na-R-ALA for neuroinflammation, blood sugar and CFS-type of issues
Pomegranate seed oil/ husk + Black Seed Oil as swiss army knifes
Lactoferrin with iron dysregulation, inflammation, gut issues,… (I would put this as a non negotiable in this protocol due to Fenton reaction fueling lipid peroxidation)
This has to be accompanied by further studies of your bloods & physiology. If you have a bottleneck within digestion, methylation, thyroid,… care for that in the first 2-6 weeks.
An exemption can be Long Covid patients as PLs seem to be very good at stabilizing the hardest cases. I would still do the prep work, but you might start slow with all of the below after 2 weeks.
If you are such a patient, priority work has to be done in these 4 domains:
Stabilizing mast cells
Lymphatic Drainage
Limbic System Retraining (like DNRS)
Rebooting the autonomic nervous system
Phase 2: True Lipid Replacement
Without any fluff here is the full stack (I will add explanations in between):
Krill Oil: 1,5-4gr
Krill oil seems to be the best option at increasing omega-3s within the membranes due to their high content of phospholipids. The amount of krill oil can vary, depending on how much fish you eat. I highly recommend checking your omega-3 index or omega 6:3 ratio (which should be 4:1).
The higher the ratio, the more you should focus on reducing PUFAs and the higher this can be. 3-7 portions of fish/ week is the minimum. If you eat “only” 3, stick to the 4gr. If you eat daily, 1,5gr is enough. Omega-3 repletion is a long term game of 3-6 months. During this stage, Vit E supplementation is highly recommended
Daily usage of high quality (tested) EVOO
Oleic acid, an omega-9 fatty acid is found within certain plasmalogens of the myelin sheet, stabilizing it. What is important to understand is this mono-unsaturated fatty acid is less prone to oxidation.
This MUFA is pro-peroxisomal health, as it itself is a potent PPAR-Alpha agonist (which I will dive in below), increasing PL synthesis. It alters lipid profile by lowering LDL and increasing HDL and can enhance endocannabinoid synthesis which is lowering pain.
I would use it as a cold drizzle on 2-3 meals per day.
Phosphatidylcholine & -serine (or a complex)
These two (& the other related phospholipids) are what make up most of our membranes apart from plasmalogens. As the show is not only about PLs, we should also use these.
Dr Neil Nathan, a pioneer within the chronic illness scene, often uses IV PC injections as says that this is a powerful treating modality for mold/ mycotoxin illness. It also supports bile production & flow, while lowering methylation needs. Choline production needs methylation groups, zapping you of many B-vitamins. Many also have genetic snippets impairing PC assembly.
One issue with P-Serine is that it should be sourced from fish (or should contain omega-3s) to not skew the ratio of omega 6:3.

In my research, P-Serine in its omega-3 form is readily available, while the P-Choline is harder to find. I would still use P-Choline in this form, as it has many benefits nonetheless.
Choline: >400mg
Once a vitamin, this molecule amazes me due to its sheer impact on liver/ detoxification physiology, bile flow and overall structural integrity of membranes.
4-6 eggs per day and weekly liver will saturate you, on top of the aforementioned P-Choline which lowers overall need beyond another supplement. I just want you to be consistent with these dietary inputs, else you will lack it.
Myo Inositol: 2-6gr
Often used as a treatment in metabolic issues, hypothyroidism and PCOS, it also increases circulating PLs through increasing head group transfer. I would not say that its a 100% inclusion, but if you suffer from any of these above, it can check multiple boxes.
PPAR Alpha Agonism for peroxisomal function
Part of this protocol, I want to include some theory again for you to understand. PPARs are a class of intracellular receptors which can act as transcription factors.
There are three main classes: alpha, gamma & delta
For this discussion, alpha will be the main focus (though all of them are very positive for you).
PPAR-Alpha is expressed within the liver, skeletal muscles, intestines, BAT, certain brain regions and kidneys. Especially the expression within the liver is important, as PPARs overall main function is to control energy metabolism & substrate usage.
If you want an overview over PPAR-Alpha, look into this table:
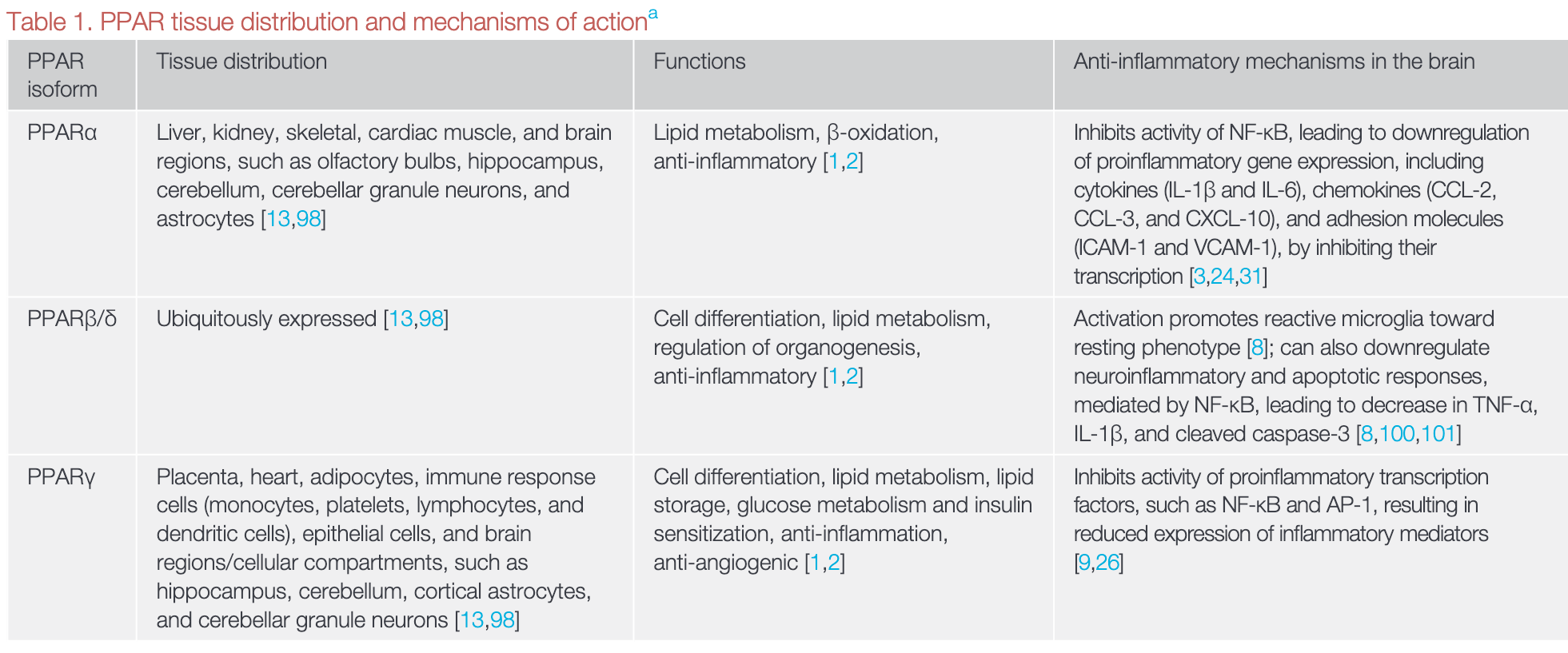
What is not included here is the fact that PPAR Alpha is one of the best levers to increase PL synthesis through modulation of peroxisomes.
Activation of PPAR Alpha → peroxisome biogenesis → increase uptake of VLCFA → increased PL output
Pretty incredible. No wonders drugs are created enhancing their function to treat neurodegenerative diseases.

Overall this reduces inflammation, improves immune cell function, membrane integrity and cellular transmission.
Now gladly there are many natural ways to improve PPAR transmisison through micronutrients, phytochemicals or endogenous compounds:
Micronized PEA
This is my personal favourite and is a potent inflammatory mediator. It lowers neuroinflammation, seals a leaky gut while reducing local inflammation and is very protective of many neurodegenerative diseases & psychological disorders. In my arsenal it has been the most potent factor in reducing brain fog.
EPA/DHA
Omega-3s can directly bind to this transcription factor and its the most potent, diet based, way to induce agonism. For diet & dosing go look back at the stuff above.
SCFAs like Butyrate or Acetate
Under normal conditions these are produced by our intestinal bacteria when fermenting fibers or certain polyphenols. As the production is often malfunctioning in people suffering from gut issues or even neurodegenerative ones, the supplementation of butyrate might be a good way to support this.
Overall this is a great link back to the study I told you about earlier:

Butyrate might act as a potent swiss army knife at restoring peroxisomal function, inflammatory & immune modulator. Huge fan of it.
To not get bored, I will give you the list of compounds with foods where you can find it that also directly agonize this transcription factor:
Oleic Acid (Avocado, EVOO)
Phytanic Acid & CLA (dairy)
Curcumin
Resveratrol
Quercetin
Naringenin (Citrus)
Rosmarinic Acid
Cinnamic Acid
Berberine
Magnolol
Gingerols (Ginger)
Mangiferin (Mango)
Through simple dietary modifications you can really add potency behind restoring peroxisomal function.
Last but not least, general dietary recommendatins & lifestyle choices are beneficial:
Ketones can act as PPAR agonists, hence why partial ketogenesis, exercise or cold plunging is beneficial
Not overfeeding (aka caloric restriction or adequacy)
Many of these above are also PPAR Gamma agonists, which is also important in driving cellular energy metabolism.
Plasmalogen Precursor Supplementation
Last but not least the most important compound which also introduced me to the whole show:
Plasmalogen precursors
The whole protocol & theory you have read led up to this compound as this is where the major difference is in most membrane replacement therapies. They are not using direct plasmalogen precursors.
There are many studies where scientists tried to find the best way to increase PLs through supplemental form and one thing always stood out:
Direct PL supplementation is inferior to other methods
This is due to our digestive tract & the respective enzymes break down the Pls before incorporation into tissues. But there are ways to circumvent this:
Alkylglycerols are direct plasmalogen synthesis precursors that bypass digestive degradation & peroxisomal assembly completely, which comes in handy if you have dysfunctional ones, and being incorporated into ER metabolism for further PL synthesis.

The enhanced absorption of AGs is due to the different chemical structure, as AGs do not have the very labile vinyl-ether (double) bond.
One way to increase plasmalogen through AGs is with Shark Liver Oil. When reading about this I was stunned to hear about this, but there are actually good studies showing increases in circulating PLs when supplementing it.
There are also studies linking it to improved immunity & cancer outcomes, which I believe is also due to the potency of PLs in improving overall immune function.
Despite that, this is not the best (rather more budget friendly) approach as these AGs are often missing the specific fatty acid at the sn-2 position, which for our purposes should be oleic acid (n-9) or DHA (n-3).
Desaturation steps at the sn-2 position still have to take place which is another bottleneck when aging or inflamed, with the added burden of not specifically incorporating these two fatty acids.
Hence why the go to option is the Prodrome Science products:
ProdromeNeuro
ProdromeGlia
Made & developed by Dr. Goodenowe one of the experts in lipid physiology, he developed these products with the added benefit of already having the specific fatty acid at the sn-2 position we want.
ProdromeNeuro = DHA (omega-3)
ProdromeGlia = Oleic Acid (omega-9)
The latter is most commonly found within the myelin sheet and has reported calming effects. Taking this as the first line approach is often the best to not excite and already inflamed system.
ProdromeNeuro is rather for immune cells and neurons changing how the latter are transmitting signals, hence why it can be quite sparking.
From what I am reading, a dosage protocol might be going like this (if you want to treat illness; this is not for maintenance):
In weeks 2-8 start ramping up ProdromeGlia to 6-10 capsules/ day.
Add in ProdromeNeuro after that with the same dosage for another 2-4 weeks. You should see changes and can go back to maintenance. During this time to get the highest ROI, get on top of the toxicities you are trying to treat.
This can be mold/ mycotoxins or candida specifically, where the practitioners are already using lipid replacement therapy, or any neurodegenerative disease already manifesting.
Note: Due to some countries having shipment issues (like my country of origin), you might use the shark liver oil, which is much less potent though.
Lipids, Peroxisomes and Plasmalogens in specific have been of utmost interest for me the past few weeks and I will try this protocol on myself, as I feel like its the future due to pandemic of Long Covid patients.
I hope you enjoyed this one.
If you want to implement this protocol into a highly specific, personalized protocol, feel free to book a call with me here to start 1:1 coaching on your most pressing health challenges.
Cheers